Glucose Intolerance & Spikes
We need to reduce glucose and insulin spikes to continue in metabolic health or return to it. This will help us prevent or reduce insulin resistance and glucose intolerance.
Metabolic syndrome is associated with glucose intolerance, higher fasting glucose and insulin levels than normal, obesity, especially an increase in visceral fat and fatty liver, and bad cardiovascular outcomes. The American Heart Association defines metabolic syndrome as being diagnosed with three or more of the following:
- Central or abdominal obesity. This is measured by waist circumference:
- Men: greater than 40 inches
- Women: greater than 35 inches
- High triglycerides: 150 mg/dL or more, or taking medicine for high triglycerides
- Low HDL cholesterol, or taking medicine for low HDL cholesterol:
- Men: less than 40 mg/dL
- Women: Less than 50 mg/dL
- High blood pressure 130/85 mmHg or more, or taking medicine for high blood pressure
- High fasting glucose (blood sugar): 100 mg/dL or more, or taking medicine for high blood glucose.
Glucose levels and spikes are controlled through a healthy diet, exercise, and weight loss. Let's look at glucose in the healthy person, impaired glucose tolerance, urine glucose, and how to control glucose spikes, which can provide insights into how to get rid of metabolic syndrome.
Glucose and Insulin in the "Normal Person" - Fasting
Consider the "normal person," someone without diabetes, metabolic syndrome, obesity, glucose intolerance, or insulin resistance.
In the morning, after an overnight fast and before any breakfast or glucose intake, how does the body get the continuous glucose it needs since the last meal from yesterday is no longer sending glucose from the intestine to the bloodstream?
This blog post is available as audio on Spotify at https://podcasters.spotify.com/pod/show/joe-breault-md-scd/episodes/Glucose-Intolerance--Spikes-e2k1re8
This is described by Sherwin:
In normal humans, after an overnight fast, the reduction in insulin concentrations to basal levels (10-15 µU/ml) results in a marked diminution of glucose uptake by insulin-sensitive tissues such as muscle and fat and the virtual total cessation of glucose uptake by the liver. Most of the glucose uptake (about 75-80%) takes place in non-insulin-dependent tissues such as the brain, the formed elements of the blood, and the adrenal medulla. Maintenance of blood glucose homeostasis in this circumstance is achieved by the release of glucose by the liver at rates equal to those of tissue utilization. The hepatic processes involved in the addition of glucose to the bloodstream consist of glycogeneolysis as well as gluconeogenesis. On the basis of studies employing splanchnic balances of gluconeogenic substrates and the rate of disappearance in liver glycogen in biopsy samples, approximately 75% of the hepatic glucose release is derived from glycogenolysis, and the remainder (25%) from gluconeogenesis (primarily by the conversion of lactate and alanine to glucose). These quantitative considerations of hepatic glucose production and peripheral glucose utilization are summarized in Figure 1.

So, in a healthy person, after an overnight fast before the first meal, 75% of the glucose needed for the body is produced by the liver breaking down glycogen (glucose that was linked together for storage in the past) and 25% by new glucose production in the liver. The liver's production of glucose in the fasting state depends on the low insulin levels (baseline levels) and the glucagon levels in the portal circulation.
How long does the normal person have to fast before the liver glycogen is used up? Murry & Rosenbloom note that average liver glycogen is 80 grams (can range up to 160 grams), so unless an average, non-exercising person is fasting for most of the day, liver glycogen can provide baseline glucose needs. After that, a different mechanism of fat burning comes into play to provide for energy needs. They also note that in intensely exercising people, muscle glycogen (larger glycogen storage of 500 grams on average) is used to fuel the muscle glucose needs.
Glucose and Insulin in the "Normal Person" - Breakfast
Once the overnight fast is broken by the day's first meal, glucose enters the bloodstream from the intestine. The increase in the blood glucose suppresses the liver production of glucose when fasting (75% breaking down liver glycogen, 25% gluconeogenesis).
Spencer notes that given a 100 mg glucose oral load, 10% of the glucose is "trapped by the liver on first passage through the portal system and never reaches the systemic circulation." Muscle and fat using insulin-dependent pathways use 15%. The brain and other non-insulin-dependent tissues use 25%. The remaining glucose is mostly taken up by the liver on subsequent passes of the circulation through the liver, where it is used to build glycogen storage and produce triglyceride and energy.
Glucose entering the bloodstream after a meal causes insulin to rise. How rapidly and how high the insulin rises depends on how rapidly and how high the glucose rises. The higher and sharper these spikes of glucose and insulin are, the more one will develop insulin resistance and impaired glucose intolerance or, if it gets worse, diabetes.
There are a number of ways to reduce these glucose spikes (easily measured by a continuous glucose monitor) and hence the insulin spikes. They include:
- Avoid overeating carbs and minimize sugars to reduce the glucose load.
- Avoid foods with sugars, especially fructose, as much as possible, except for whole fruit (https://www.healthyinsight.org/toxic-fructose/).
- Avoid ultra-processed foods.
- Before ingesting a carbohydrate load, partly block the rapid absorption of glucose in the duodenum by laying down a mesh of insoluble fiber and filling the gaps with soluble fibers. One way to do this is to eat vegetables before carbohydrates. This also allows the glucose to pass further down into the small intestine and feed the microbiome as it slows down glucose absorption.
- Another way to partly block the rapid absorption of glucose and send it further down the intestine to feed the microbiome is to have a few teaspoons of vinegar in a large glass of water before a carbohydrate meal. Sucrose is a molecule of glucose and fructose linked together. Starches are glucose molecules linked together. These are broken down in the intestine by enzymes that appear to be slowed down by vinegar (the mechanism is complex; see https://academic.oup.com/nutritionreviews/article/72/10/651/1935511). This allows glucose to go further down the intestine to feed the microbiome rather than getting quickly absorbed in the duodenum.
- Another way to partly block the rapid absorption of glucose from a heavy carbohydrate meal is by adding fiber and healthy fat. For example, when cooking a serving of oatmeal, add a dozen almonds and a few teaspoons of olive oil.
- Walk or exercise after a meal for 10-20 minutes.
Impaired Glucose Tolerance
The mechanism for glucose being transported into body tissues is via cell wall proteins in the GLUT family. This is facilitated diffusion, where glucose is transported by cell wall GLUT proteins from the high concentration of glucose in the blood to the low concentration in the body tissues, such as muscles. "the amount of glucose that can diffuse in the cells is limited except for liver and brain cells.... This diffusion is significantly increased by insulin to 10 times or more." An exception is the GI tract and kidney, where "glucose is transported actively by sodium-glucose co-transport against the concentration gradient." (reference)
Once glucose diffuses into muscles and other body tissues, it gets phosphorylated, locking it into the cell and preventing it from diffusing out. The glucose inside the cell can be used to produce energy (ATP via glycolysis) or stored as glycogen.
Insulin is needed for the transport of glucose into muscle and fat. However, as a person becomes unhealthy (metabolic syndrome), the transport of glucose into the cells gets harder because the transport mechanisms become less sensitive to insulin. As a result, the glucose in the bloodstream increases, and the pancreas pushes more insulin to overcome insulin resistance. Eventually, both the fasting sugar and insulin levels will become higher than normal. This is impaired glucose tolerance and insulin resistance, which may progress eventually to diabetes.
Using the tips above to keep insulin spikes lower can help prevent or delay metabolic syndrome, and it can also help reverse it.
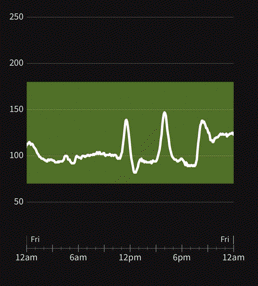
Oxyhyperglycemia is a special type of impaired glucose tolerance with a normal fasting sugar. It is characterized by a rapid glucose spike after a meal, where the peak is high enough to cause transient, symptom-free glucose in the urine. The spike reverses rapidly with a sharp downstroke overshooting towards a low blood sugar. This also triggers a sharp insulin spike that, when repeated over a long period, leads to metabolic syndrome. The tips above can moderate the peaks.
Urine Glucose
If blood sugar levels are too high, the kidneys cannot reabsorb the sugar from the urine back into the blood, and the sugar leaks out into the urine. Sugar in the urine is called glycosuria. This is common in uncontrolled diabetes, and in pre-modern times, a doctor tested for diabetes mellitus by seeing if the urine tasted sweet. The interesting biochemistry and transporters involved are detailed here.
The renal threshold is the level of a substance that is too high in the blood and spills over into the urine. Here, we are only discussing the renal threshold for glucose. A 2021 study in China graphed how the renal threshold of glucose (RTG) varies based on HgbA1c (a 3-month average of blood glucose):

You likely had an HgbA1c blood test during your last annual exam, so the above graph can help you estimate your renal threshold for leaking glucose into the urine. A 2017 Publication (Chapter in a reference textbook) claimed that RTG in healthy subjects is about 180 mg/dl of glucose vs up to 240 mg/dl in diabetics, but multiple other publications note that this can vary widely. If you have a continuous glucose monitor and urine test strips for glucose, you can experiment on yourself to see what your renal threshold is.
Reduce Glucose Spikes
Reducing glucose spikes will reduce insulin spikes, which in turn will reduce glucose intolerance and insulin resistance or prevent them. This means that the glucose in your bloodstream can be transported into tissues with a lower insulin level, which helps with the transport. Thus, the tissue and muscle mitochondria can burn the glucose more effectively, providing more energy, less fatigue, and less chance of diabetes and metabolic syndrome developing.
A calorie deficit is one aspect of losing weight and preventing metabolic syndrome. Massive overeating, where "calories in" far exceed "calories out," is not a winning combination. But a calorie is not a calorie.
The types of foods we eat make a major difference in our health and weight, even controlling for calories. Sugars (except in whole fruit) do us more harm than good, especially fructose, and so should be avoided or limited. When we eat carbohydrates, the more the absorption in the duodenum can be postponed, so the sugars go further down the intestine to feed the microbiome, and slow glucose absorption, the better. This can be accomplished by having fiber (vegetables) and a few teaspoons of vinegar in a glass of water before the carbohydrates. Walking after a meal also helps.
Protein digestion is inefficient. It uses up more energy (calories) in heat (25-30%) than in carbohydrate digestion (6-8%). One study showed that in a high-protein, carbohydrate-free diet, "Forty-two percent of the increase in energy expenditure ... was explained by the increase in gluconeogenesis. The cost of gluconeogenesis was 33% of the energy content of the produced glucose." So, one-third of the calorie energy in the protein that was changed into glucose was used to create the glucose. If you eat the same calories in sugar, very little of the calories are used to create glucose.
When we keep the glucose spikes low, eat enough protein, avoid ultra-processed foods and sugars, and consume unprocessed carbohydrates with lots of fiber, the hormones controlling our appetite and hunger work well. It becomes easier to limit our eating with reduced cravings.